The Project Gutenberg eBook of A Bilateral Division of the Parietal Bone in a Chimpanzee; with a Special Reference to the Oblique Sutures in the Parietal
most other parts of the world at no cost and with almost no restrictions
whatsoever. You may copy it, give it away or re-use it under the terms
of the Project Gutenberg License included with this ebook or online
at www.gutenberg.org. If you are not located in the United States,
you will have to check the laws of the country where you are located
before using this eBook.
Title: A Bilateral Division of the Parietal Bone in a Chimpanzee; with a Special Reference to the Oblique Sutures in the Parietal
Author: Aleš Hrdlička
Release date: October 19, 2010 [eBook #34101]
Most recently updated: January 7, 2021
Language: English
Credits: Produced by Larry B. Harrison and the Online Distributed
Proofreading Team at https://www.pgdp.net
*** START OF THE PROJECT GUTENBERG EBOOK A BILATERAL DIVISION OF THE PARIETAL BONE IN A CHIMPANZEE; WITH A SPECIAL REFERENCE TO THE OBLIQUE SUTURES IN THE PARIETAL ***
A Bilateral Division of the Parietal Bone
in a Chimpanzee; with a Special Reference
to the Oblique Sutures in the
Parietal.
By Aleš Hrdlička
AUTHOR'S EDITION, extracted from BULLETIN
OF THE
American Museum of Natural History,
Vol. XIII, Article XXI, pp. 281–295.
New York, Dec. 31, 1900.
The Knickerbocker Press, New York
[Pg 281]
Article XXI.—A BILATERAL DIVISION OF THE
PARIETAL BONE IN A CHIMPANZEE; WITH
SPECIAL REFERENCE TO THE OBLIQUE SUTURES
IN THE PARIETAL.
By Aleš Hrdlička.
The first to describe a case of division of the parietal bone in
apes was Johannes Ranke, in 1899.
[1] The skull in question is
that of an adolescent female orang, one of 245 orang crania in
the Selenka collection in the Munich Anthropological Institute.
The abnormal suture divides the right parietal into an upper
larger and a lower smaller portion. "The suture runs nearly
parallel with the sagittal suture," but, as the illustration shows
(Fig. 1), it descends in its posterior extremity towards the temporo-parietal
suture, and terminates in this a few millimetres in
front of the lambdoid suture. The abnormal suture shows but
little serration, and the articulation of the two divisions of the
parietal bone is squamous in character, the lower portion overlapping
the upper. Below the junction of the abnormal with the
coronal suture, the latter takes a pronounced bend forward. A
similar bend in the coronal suture is present in the same specimen
on the left side. This is common among the other orang
skulls in the collection. The portions of the coronal suture below
and above the bend differ somewhat in character.
Besides the above-mentioned complete division, Ranke found
among the 245 orang skulls 13 with incomplete division of the
parietal bone. The division consisted invariably of a longer or
shorter remnant of a horizontal "parietal suture," ending in the
coronal suture at the top of the bend above referred to. A similar
anterior remnant of an abnormal parietal suture was found by
Ranke in a young chimpanzee skull; but the author questions
the word "chimpanzee," which evidently means that the identity
of the skull is somewhat doubtful.
In consequence of his finds, Ranke believes both complete
and incomplete divisions in the parietal bone to be much more
[Pg 282]
frequent in the orang than in man.
[2] He also thinks that the
bend usually present in the coronal suture in the orang signifies
that, "even where there are no traces of a parietal suture, such a
suture has actually existed in an earlier stage of development."
This implies the development of the adult parietal bone in the
orang from two original
segments, one
above the other.

Fig. 1. Division of the Right Parietal in an Orang
(Ranke, Abh. d. k. bayer. Akad. d. Wiss., II cl., XX Bd., ii Abth.).
The divisions which
I am about to describe
occur, one in
each parietal, in the
skull of a nine-year-old
male chimpanzee,
which was captured,
when young, in West
Africa. Later on he
was one of the attractions
of the Barnum
and Bailey Circus,
and was familiarly
known as Chico. The
chimpanzee died in 1894, since when his skin and bones have
been preserved in the American Museum of Natural History,
New York City. Prof. J. A. Allen, the curator of the Zoölogical
Department of the Museum, has kindly given me permission to
describe the skeletal parts for publication.
[3]
The most interesting part of Chico is unquestionably the skull.
The divisions of the parietal bones which the specimen presents
are not only the first complete divisions of the parietal observed
in a chimpanzee, but are also unique in character, no divisions of
the same nature having been observed before, either in man,
in apes, or in monkeys. The position and extent of the divisions
in this skull will throw considerable light on the question of the
[Pg 283]
aberrant, complete divisions of the parietal bone, by which term
may be designated divisions differing from the typical horizontal
ones.
The skull under consideration shows in general a good development
and an almost perfect symmetry. The capacity of the
brain cavity, measured according to Flower's method, is 390 c.c.
The masculine features of this skull, and particularly the
temporal ridges, are not quite as marked as those of another
skull of an adolescent male chimpanzee in the Museum. The
temporal ridges are slightly prominent, and in their middle third,
over part of the frontal and the parietal bones, not more pronounced
than in some human crania. They are, however, situated
very high. Their upper lines or boundaries touch each other
over a part of the sagittal suture, a little back of the bregma;
while the lower lines approach to within 6 mm. of the sagittal
suture. The supraorbital ridges are not very massive, although
prominent to such a degree that, when the skull rests on
the occipital condyles and on the teeth, the plane of the orbits is
almost vertical. The sagittal crest is insignificant; the occipital
crest is high, but not very massive. The zygomatic arches are less
strong than they are in an average white male; and the mastoids
are small, even smaller than in an average adult white female.
The second dentition is incomplete; the third molars have not
reached the level of the opening of their sockets. The condition
of the sutures, so far as their patency is concerned, does not
bear the same relation to the stage of dentition as it does in
man: all the sutures of this skull are more or less obliterated.
There are no signs on any part of the skull that point to the
closure of any of the sutures as premature. In detail, the condition
of the sutures is as follows: The spheno-maxillary articulation
is completely closed, but still plainly traceable. Of the
various facial sutures, only remnants are open; the suture in the
zygomatic arch, however, is almost fully patent on both sides.
The spheno-frontal articulation is completely obliterated on the
left, but traces of it remain on the right side. The left temporo-sphenoidal
and squamo-frontal sutures (the squama of the temporal
articulates with the frontal bone) are, with the exception of
the basal part of the former, which remains open, quite obliterated,
but on the right side both are open. The temporo-parietal
[Pg 284]
sutures, with the exception of 8 mm. of the anterior end of
the suture on the right side, are both entirely closed and hardly
traceable. The coronal suture is partly open on the left, and
wholly open on the right, up to a point a little below the middle
of the anterior border of the parietal bone. At this point on each
side, the lower portion of the coronal suture bends backward
and continues as the anomalous suture; the upper portion of
the coronal, particularly on the right, is completely obliterated,
though still traceable. There are no signs left of the sagittal
and lambdoid sutures, and only the basal portions of the temporo-occipital
articulation remain. The palatine sutures, also, are
entirely obliterated.
The skull shows no important anomalies besides the division
of the parietals.
The divisions of the parietal bones begin on the left 32 mm.,
on the right 28 mm. (measured with a tape), above the point of
junction of the coronal and temporo-parietal sutures. From the
point where the anomalous sutures leave the coronal suture, to
the bregma, the distance on the left is 44 mm., on the right
42 mm. The excess of size of the left over the right parietal
bone along the coronal suture (6 mm.) compensates the greater
height of that portion of the right temporal squama which articulates
with the frontal bone. Measured across their middle from
the temporo-parietal suture, the two parietals appear to be almost
of equal size (left 82 mm., right 80 mm.). In an antero-posterior
direction, from the beginning of the division to the middle of the
parietal portion of the occipital crest, both bones measure the
same, namely 75 mm.
The division in the left parietal begins at a V-shaped cleft,
which is filled with a process of the frontal bone. There are
slightly distinct markings on the bone and a number of insular
ossicles, which make it probable that the cleft had been originally
much greater and was largely filled by a Wormian or, rather, a
fontanel bone, the lower border of which has subsequently united
with the parietal.
For 30 mm. from its beginning the abnormal suture proceeds
directly backward, and to this extent shows but little obliteration.
The original cleft has, it seems, extended up to this point.
From here the suture takes a slight bend upwards, and proceeds
[Pg 285]
[Pg 286]
almost directly upwards and backwards, becoming gradually obliterated,
until it disappears at the temporal ridge, 16 mm. from
the median line. Originally the suture must have terminated on
the posterior border of the parietal bone, not far from the
lambda. The whole suture shows fairly good serration. The
coronal suture on this side, below the division, shows serration
about equal to that of the abnormal suture; the obliterated portion
above this was, so far as can be seen, more simple.
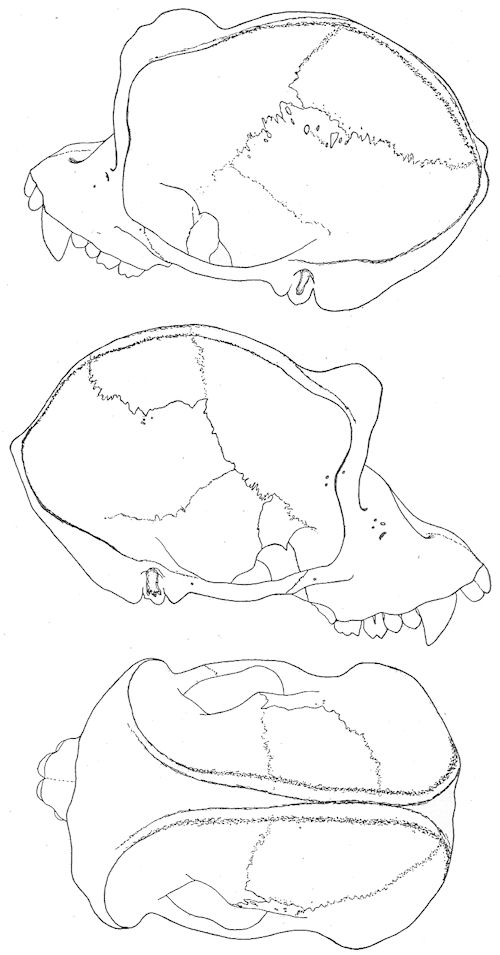
Figs. 2–4. Skull of an Adolescent Male Chimpanzee.
On the right side the division of the parietal may also have
begun with a cleft in the anterior border of the bone, but, owing
to the advanced state of obliteration of the upper portion of the
coronal suture on this side, the existence of the cleft cannot be
fully ascertained. Here also the abnormal suture, at first wholly
open, runs for the first 26 mm. directly backwards; at this point
the suture, still quite patent, takes a turn somewhat sharper
than that on the left, and proceeds for 16 mm. backwards and upwards;
here it takes a second turn, and proceeds almost directly
upwards towards the sagittal suture. This last portion of the
abnormal suture is considerably obliterated, and on and beyond
the temporal ridge is scarcely traceable. The point at which the
division has reached the sagittal suture is situated a little behind
the middle of the latter. The abnormal as well as the open
part of the coronal suture on this side shows a simpler serration
than the corresponding sutures on the left side.
In this specimen there is on neither side any encroachment of
the lower portion of the parietal bone upon the frontal, such as
Ranke lays stress on in the case of his orangs. A second skull of
an adolescent male chimpanzee, in the Museum of Natural History,
has a decided bend in the coronal suture, not unlike that
which Ranke describes, and which, as he thinks, generally indicates
an old parietal division; but in this case the bend is situated
between the inferior and superior boundaries of the prominent
temporal ridge, and apparently owes its origin to the latter (Figs. 2, 3, 4).
The main interest in the case just described centres in the
direction of the abnormal sutures, and in the clearness with which
the two divisions appear as equivalent and of the same origin,
although one divides the parietal completely, while the other is
restricted to one of its angles.
[Pg 287]
As to the course of the abnormal suture in the parietal bone,
in all the cases thus far reported, the division runs in a horizontal
direction (cases of Tarin, Soemmering, Gruber, Hyrtl, Welcker,
Turner, Putnam, Dorsey, Ranke, and others); or it runs obliquely
from or near the middle of the lambdoid suture to some
part of the temporo-parietal suture, the sphenoidal angle, or the
lower portion of the coronal suture (cases of Curnow, Ekmark,
Gruber, Hyrtl, Lucae, Welcker, Putnam, Traquair, Ranke); in
a case of Simia silenus described by Gruber and in an Egyptian
cranium described by Smith, the divisions run to the lambda
and begin respectively slightly above the pterion and at it. In
Boyd's and in two of Hyrtl's cases, the abnormal suture begins
at or below the bregma on the coronal margin of the parietal
bone, and ends at or near its mastoid angle; finally, in Blumenbach's
(cited by Welcker), Bianchi's, Fusari's, and Coraini's cases
(those of Coraini include two monkeys) the division is vertical,
passing between the temporo-parietal and sagittal sutures. The
left division in our chimpanzee approaches those in Gruber's
Simia silenus and Smith's cases; but it originates much higher
anteriorly, and terminates slightly below the lambda on the occipital
border of the parietal. The division in the right parietal of
the chimpanzee, beginning slightly below the middle of the anterior
border of the bone, and ending slightly back of the middle
of its sagittal border, has no analogy among the cases previously
described.
The difference in extent and terminations of the two abnormal
sutures in the chimpanzee is of particular interest in connection
with the problem of the significance and origin of those divisions
of the parietal bone that involve more or less only one of its
angles.
Since the observations of Toldt,
[4] and more recently of Ranke,
[5]
on the development of the parietal bone in the human embryo, it
appears, though it cannot as yet be said whether the fact is or is
not general, that the bone originates from two centres of ossification.
These centres appear in most cases one directly above the
other, but, as Ranke himself shows,
[6] and as can hardly be otherwise,
these primitive components of the parietal do not always
[Pg 288]
show the same relations in size or position. The centres blend
together, ordinarily, at the end of the third or during the first
half of the fourth month of fœtal life. On this account, the
typical, complete, horizontal division of the human parietal bone,
when met with at any time after the fourth month of fœtal life,
is generally interpreted to-day as a retardation of the union, or a
persistence of separation, of the two original segments of the
bone. Opinion, however, is still unsettled as to the significance
of the more atypical, oblique divisions of the parietal, particularly
of those where the separation is limited to one angle. Up to the
recent contribution on the subject by Ranke, the weight of opinion
on the point, although rather briefly expressed, seems to have been
in favor of attributing to these smaller, oblique divisions, the
same significance as was given to the more typical, horizontal
ones. Gruber,
[7] in reporting a new case of a bilateral oblique
suture in the parietal bone, calls the separated mastoid angles
"the secondary posterior parietals." Hyrtl and Welcker advance
no definite theories on this point, though the latter expresses an
opinion
[8] that in both the horizontal division and the separation
of the mastoid angle of the parietal bone the development of the
condition may be identical. In 1883 Prof. F. W. Putnam, in
describing one of his Tennessee skulls with an abnormal oblique
suture in each parietal,
[9] referred the development of the separated
mastoid angle on the right side, as well as the larger oblique
inferior portion of the parietal on the left side, to a "separate
centre" of ossification. Ranke
[10] opposes both Gruber's and
Putnam's opinion, and presents instead a theory somewhat vague
and not satisfactorily demonstrated, by which he accounts for
the origin of oblique sutures from partial horizontal sutures in
the parietal bone through "half-pathological processes." In his
words, "the oblique parietal suture is allied to the half-pathological
conditions of the skull; it is wholly unjustifiable to
speak, as W. Gruber has done, of a separate Parietale secundarium
posterius, severed by the suture, as of a typical, in a certain sense
normal, formation. The oblique parietal suture is nothing more
[Pg 289]
than an incomplete (posterior), true, i. e., typical, parietal suture
with a sagittal course, modified by certain half-pathological conditions."
These half-pathological conditions are produced, the
author explains on the preceding page, "durch Einknickung der
nach Herrn G. H. Meyer 'plastisch' aufwärts gebogenen hinteren
Scheitelbeinränder."
This opinion of Ranke calls for a few words about the incomplete
horizontal parietal sutures. These sutures are apparently
very rare in human adults, only five instances being on record
(4 Ranke's, 1 Turner's). They are more frequent in orangs
(Ranke), and quite common (as Ranke shows, and as I found
independently before Ranke's publication of his observations)
in the human embryos near term and in new-born or very young
infants. In the human family, these partial divisions of the
parietal generally begin in the posterior part, and run sagittally
to the posterior border of the bone, ending in this border at or
near its middle. In orangs the incomplete horizontal divisions
seem to begin, as a rule, in the anterior part, and end at or
near the middle of the anterior border of the parietal. The
length of these divisions varies from a few millimetres to several
centimetres, and they even reach up to the centre of the parietal
bone.
[11] These divisions are, without doubt, the remains of the
original anterior and posterior clefts, or, if we go a step further,
of the original intervening antero-posterior space between the
original inferior and superior segments of the parietal. From
the very first contact of the growing centres, the median extremity
of these clefts is bounded both below and above by a
mass of bone; and when the anterior or posterior border of the
parietal comes finally in contact with the frontal or occipital
bone, the anterior and posterior sagittal clefts, if they still exist,
lie between two well-developed, firm portions of the bone. Under
these circumstances it is quite impossible to imagine any
disturbance, mechanical or pathological, that could affect solely
or mainly the median portion of the cleft, and cause a deflection
downward in this portion of the division, or cause its extension
to the inferior border or even the anterior-inferior angle of the
parietal.
There are only two factors that can possibly affect and modify
[Pg 290]
the course of the incomplete parietal suture, and both of these
would show their influence mainly or entirely on the distal
portion of the same. These two factors are, first, an abnormal
development, either defective or excessive, of one of the original
parietal segments; and, secondly, influences that would interfere
with the freedom of full growth of the anterior or posterior
border of the parietal.
In the first case, as can easily be imagined or even artificially
demonstrated, there would be possible only a lower or higher
situation or an obliquity affecting mostly the marginal portion of
the division. The results would be low or high sagittal sutures,
and curved or oblique sutures diverging from the parietal eminence,—effects
entirely different from the actually observed
oblique sutures that sever the lower portion of the parietal, or its
mastoid angle.
Influences interfering with the free development of the anterior
or posterior border of the parietal bone could only deflect upwards
or downwards the marginal end of an incomplete parietal
suture, or, at most, in a case of a short suture, render it oblique
or curved in its entirety. No pathological condition, unless it were
accompanied by a fracture, could extend even a deflected antero-posterior
incomplete division to any of the borders of the bone.
There are, it seems to me, only three possible ways in which an
oblique suture, extending between any two borders of the parietal
bone, can be produced.
In the first case the oblique suture, or rather a suture-like formation,
may be the effect of an early fracture. A fracture produced
in adult life is generally recognizable as such; but a
fracture dating from earlier stages of life, produced before the
growth of the bone has ceased, may, if not entirely obliterated,
present more or less the characteristics of a suture. I have seen
several skulls where a division in the parietal bone or the temporal
squama presented at the same time features of a fracture
and suture; in one or two of these cases so much so, that it was
and still is impossible for me to decide exactly which of the two
conditions I had before me. Gruber describes one such case
[12]
as an instance of an oblique parietal suture, while Hyrtl and
Ranke both consider this case as one with an acquired division.
[Pg 291]
To differentiate a congenital real oblique suture from a division
which is the result of a fracture, we must be guided largely by
the situation, form, and serration of the division, and the condition
of the surrounding bones, especially that of the opposite
parietal. A straight course, ending with one extremity in or
near the middle of the anterior or posterior border of the parietal,
a complex serration, no continuity of the division on the neighboring
bones, and particularly a co-existence of an allied or
similar division on the opposite parietal,—all favor the conclusion
that the division under consideration is a real congenital
suture, and not the result of a fracture.
In the second case there are reasons for believing that an
oblique suture of the parietal bone can originate in the same
way as the horizontal one, namely, through a persistence of the
original separation between the two centres from which the bone
is developed, and a co-existent difference in the relative position
or the relative growth of the two centres. It is in this connection
that the above-described division in the parietals of the chimpanzee
will prove of value.
The occasional persistence of the separation between the two
original segments of the parietal bone is sufficiently demonstrated
by the presence of the complete horizontal parietal suture. Differences
in the relative position of these segments can be observed
in a limited degree in Ranke's illustrations of embryos,
before referred to; it can be deduced from such cases as the two
of Hyrtl,
[13] in which the division of the parietal was directed from
the upper portion of the anterior to the lower portion of the posterior
border of the bone. The most pronounced change in the
position of these centres may be witnessed in cases where the
parietal bone shows a perfect vertical instead of a horizontal suture.
Such cases have been referred to before, and I presented
at the meeting of the Association of American Anatomists, in
1899, several such examples, found by me in skulls of monkeys
in Professor Huntington's anatomical collection in the Medical
Department of Columbia University. One of these specimens is
shown in the accompanying illustration (Fig. 5).
A difference in the relative growth of the two centres of the
[Pg 292]
parietal bone is well shown in the difference of size between the
inferior and superior portions of the parietal in cases of the complete
horizontal suture in the same. In the majority of such
cases on record the superior portion is larger, particularly anteriorly,
than the inferior; so
much so, that that condition
seems to be the typical one.
The difference in the size of
the two portions of the parietal,
and in their relative anterior
and posterior height, is most
pronounced in one of Gruber's
cases,
[14] where the "parietal suture"
begins only 10 mm. above
the pterion, and ends 40 mm.
above the asterion. In Dorsey's
case
[15] the lower portion
of the divided parietal is 12
mm. higher than the upper.
The same condition as is found
in Gruber's case, here mentioned,
exists in the almost
identical left division of the second case of Putnam, of
which I have a photograph in my hands. A somewhat similar
excess of the posterior over the anterior part of the lower severed
portion of the parietal can also be seen in the illustrations of the
cases of Tarin, Lucae, and Turner (Admiralty Islands skull). In
Calori's interesting case
[16] there is a decided excess of the lower
portion of the divided parietal in its posterior portion on the left
and in its anterior portion on the right side.

Fig. 5. Macacus rhesus (Medical Department,
Columbia University), showing a Complete Division of the Right Parietal Bone in
a Vertical Direction.
In case the upper segment was not vertically above the lower
one, but in a position a little more forward or backward of it;
and, furthermore, if the relative growth of the two segments
differed, and their separation remained permanent,—the separation
of any portion of the parietal bone in almost any form and
to almost any extent might result. Such coincidence of anomalous
[Pg 293]
conditions, although necessarily rare, cannot, from what
we know on the subject in parietal and other bones, be declared
improbable. All cases where oblique suture on one side
co-exists with more or less horizontal suture on the other
side in the parietal bone, as in the second of Putnam's cases,
would of course point directly to a similar origin of the anomaly
on both sides of the cranium. That such cases have not been
more frequently observed is largely due, I think, to the rarity of
bilateral parietal divisions.
A third mode of development of the oblique suture in the
parietal bone suggests itself where the severed portion of the
bone is small, and that is the possible existence of a supernumerary,
third centre of ossification. I am by no means ready
to defend this theory, yet there are cases in which it would afford
the easiest explanation. I have a Peruvian skull at hand, in
which there is a bilateral, quite symmetrical quadrangular separate
piece of bone, encroaching on the mastoid process of the parietal.
The surface of the left parietal bone in this skull measures across
its middle in antero-posterior direction 120 mm., in infero-superior
direction 130 mm.; similar measures of the right parietal are respectively
117 and 130 mm. The separate bone on the left
measures across its middle in
antero-posterior direction 20
mm., in infero-superior
direction 12 to 21 mm.; the
same portion on the right
measures respectively 25 and
11 to 15 mm. Both pieces are
joined to the parietal bone by
a squamous suture (Fig. 6).
Fig. 6 (99/3550). Quadrilateral Fontanel Bones
in a Peruvian Male Skull, encroaching upon the
Mastoid Angle of the Parietals.
It is apparent that the separate
pieces of bone in this
case are too small to be easily
taken for representatives of
one of the regular centres of
ossification of the parietal
bone; but the same pieces are somewhat too large, and
especially too singularly outlined and joined to the parietal, to be
without difficulty diagnosed as simple Wormian or fontanel
[Pg 294]
bones. One of Ranke's cases,
[17] though the separation of the
mastoid angle is oblong instead of quadrangular, as in the Peruvian
skull, seems to me to present a similar difficulty in properly
diagnosing the nature of the severed portion. This group of
cases needs further observation, particularly on the bones of infants
and embryos. I have two monkey skulls at hand which
actually show a multiplicity of the original segments of the parietal.
These specimens will be described in a future publication.
So much as to the formation of the oblique sutures in the parietal.
It should not be forgotten that such sutures can be simulated
by those which divide true Wormian or fontanel bones from
the parietal. The distinction between the real oblique parietal
and these extra-parietal sutures must depend largely on the extent
of the division and form of the separate piece of bone.
We may now return to the skull of our chimpanzee. In considering
the nature of the divisions in the parietal bones of this
skull, we can at once and absolutely discard the idea of the
divisions being due to fractures, or being boundaries of
Wormian or fontanel bones, and thus really extra-parietal in
their nature. There is nothing about the sutures, or the divided
pieces, or the neighboring bones, that would even suggest such
an explanation; and in our records on Wormian and fontanel
bones we find no analogies either in man, or apes, or lower animals,
to the conditions here observed. The necessary conclusion
from this can only be that we have before us two examples of
real parietal division.
The division on the left side, had it existed alone, would be
readily acceptable as an instance of the "parietal suture." The
anterior extremity and more than the anterior third of the course
of the division correspond exactly to the same features of a
typical, horizontal "parietal suture;" while the elevation of the
posterior extremity of the division, though unusual, can readily
be explained as due to an excess in growth of the inferior original
centre of the bone, which may, in addition, have been situated
slightly posterior to the upper centre.
The division in the right parietal of the chimpanzee begins at
its anterior end, and runs for the first third of its course in the
same way as that on the left side; its posterior end, however,
[Pg 295]
does not reach the lambdoid, but turns up and ends in the sagittal
border. Should this formation have existed alone, I should
be inclined to consider it either as the result of an accessory
centre of the parietal, or, possibly, as a persistence of the anterior
portion of the divided superior centre of the bone, the posterior
portion of the same being united with the lower segment of the
parietal in the usual way. With the division of the left parietal
in the same skull before me, everything points to a similar origin
of the division on both sides, and to the right as well as the left
division being a true "parietal suture," deflected less on the
left and more on the right side by a disproportion in growth of
the two original, regular segments of each of the bones.
The disproportion of growth of the two original segments of
the parietal bone will, I believe, be found more common as attention
is directed to this subject. It can be well explained,
though there may at times be other factors present, by a difference
in the blood-supply to the two centres. This of course may
occur not only in different skulls, but also on the two sides of
the same cranium.
Footnotes
[1] Die überzähligen Hautknochen des menschlichen Schädeldachs, Abh. d. k. bayer. Akad.
d. Wiss., II Cl., XX Bd., II Abth., pp. 36 et seq., Fig. 17.
[2] L. c., p. 41. Among 3000 Bavarian crania, Ranke found but one with complete and three
with incomplete parietal sutures; basing his conclusion on this observation, he says, "Bei den
Orangutanschädeln ist die Häufigkeit der Scheitelbeinnäthe circa 40 mal grösser als bei
dem erwachsenen Menschen."
[3] Since finding the abnormal sutures on this skull, I have been able to present the same at a
meeting of the Association of American Anatomists (1899) and before the Ethnological Society
of New York City (1900).
[4] Toldt, C., in Maska's Hdb. d. gerichtl. Med., 1882, v. III, p. 515; the same in his U.
d. Entwick. d. Scheitelbeins d. Menschen, Zeitschr. f. Heilkunde, 1883, v. IV, pp. 83–86.
[5] L. c., pp. 324–330.
[6] L. c., pp. 327–330, Figs. 29–32.
[7] Gruber, W., Beobacht. a. d. menschl. u. vergl. Anat., Berlin, 1879, II Heft, pp. 12–15.
[8] Welcker, H., Untersuch. ü. d. Wachsthum u. Bau d. menschl. Schädels, Leipzig, 1862,
p. 109.
[9] Putnam, F. W., Abnormal Human Skulls from Stone Graves in Tennessee (Proc. A.
A. A. S., XXXII, 1884, p. 391).
[10] L. c., p. 309.
[11] Ranke's Fig. 25, p. 318.
[12] Virchow's Archiv, 1870, v. 50, p. 113.
[13] Hyrtl, J., Die doppelten Schläfenlinien d. Menschenschädel, etc. (Denkschr. d. math. naturw.
Classe d. k. Akad. d. Wiss. zu Wien, 1871, v. XXXII, pp. 39–50).
[14] Gruber, W., Beobacht. a. d. menschl. u. vergl. Anat., Berlin, 1879, II Heft, p. 15.
[15] Dorsey, G. A., Chicago Med. Recorder, v. XII, Feb., 1897.
[16] Calori, Luigi, Sut. soprannum. d. Cranio Umano (Mem. d. Accad. d. Sc. d. Ist. d. Bologna,
1867, pp. 327 et seq., Fig. 4).
[17] L. c., p. 303, Fig. 13.
PUBLICATIONS
OF THE
American Museum of Natural History
The publications of the American Museum of Natural History consist of
the 'Bulletin,' in octavo, of which one volume, consisting of about 400 pages,
and about 25 plates, with numerous text figures, is published annually; and
the 'Memoirs,' in quarto, published in parts at irregular intervals.
The matter in the 'Bulletin' consists of about twenty-four articles per
volume, which relate about equally to Geology, Palæontology, Mammalogy,
Ornithology, Entomology, and (in the recent volumes) Anthropology.
Each Part of the 'Memoirs,' forms a separate and complete monograph,
with numerous plates.
MEMOIRS.
Vol. I (not yet completed).
Part I.—Republication of Descriptions of Lower Carboniferous Crinoidea
from the Hall Collection now in the American Museum of Natural History,
with Illustrations of the Original Type Specimens not heretofore
Figured. By R. P. Whitfield. Pp. 1–37, pll. i-iii. September 15, 1893.
Price, $2.00.
Part II.—Republication of Descriptions of Fossils from the Hall Collection in
the American Museum of Natural History, from the report of Progress for
1861 of the Geological Survey of Wisconsin, by James Hall, with Illustrations
from the Original Type Specimens not heretofore Figured. By
R. P. Whitfield. Pp. 39–74, pll. iv-xii. August 10, 1895. Price, $2.00.
Part III.—The Extinct Rhinoceroses. By Henry Fairfield Osborn. Part I.
Pp. 75–164, pll. xiia-xx. April 22, 1898. Price, $4.20.
Part IV.—A complete Mosasaur Skeleton. By Henry Fairfield Osborn. Pp.
165–188, pll. xxi-xxiii, with 15 text figures. October 25, 1899.
Part V.—A Skeleton of Diplodocus. By Henry Fairfield Osborn. Pp.
189–214, pll. xxiv-xxviii, with 15 text figures. October 25, 1899. Price
of Parts IV and V, issued under one cover, $2.00.
Vol. II. Anthropology (not yet completed).
The Jesup North Pacific Expedition.
Part I.—Facial Paintings of the Indians of Northern British Columbia. By
Franz Boas. Pp. 1–24, pll. i-vi. June 16, 1898. Price, $2.00.
Part II.—The Mythology of the Bella Coola Indians. By Franz Boas. Pp.
25–127, pll. vii-xii. November, 1898. Price, $2.00.
Part III.—The Archæology of Lytton, British Columbia. By Harlan I.
Smith. Pp. 129–161, pl. xiii, with 117 text figures. May, 1899. Price, $2.00.
Part IV.—The Thompson Indians of British Columbia. By James Teit.
Edited by Franz Boas. Pp. 163–392, pll. xiv-xx, with 198 text figures.
April, 1900. Price, $5.00.
Part V.—Basketry Designs of the Salish Indians. By Livingstone Farrand.
Pp. 393–399, pll. xxi-xxiii, with 15 text figures. April, 1900. Price, 75 cts.
Vol. III. Anthropology (not yet completed).
Part I.—Symbolism of the Huichol Indians. By Carl Lumholtz. Pp. 1–228,
pll. i-iv, with 291 text figures. May, 1900. Price, $5.00.
BULLETIN.
| Volume | I, 1881–86 | Price, $5.50 |
| " | II, 1887–90 | " 4.75 |
| " | III, 1890–91 | " 4.00 |
| " | IV, 1892 | " 4.00 |
| " | V, 1893 | " 4.00 |
| " | VI, 1894 | " 4.00 |
| " | VII, 1895 | " 4.00 |
| " | VIII, 1896 | " 4.00 |
| " | IX, 1897 | " 4.75 |
| " | X, 1898 | " 4.75 |
| " | XI, Part I, 1898 | " 1.25 |
| " | II, 1899 | " 2.00 |
| " | XII, 1899 | " 4.00 |
For sale by G. P. Putnam's Sons, New York and London;
J. B. Baillière et Fils, Paris; R. Friedländer & Sohn, Berlin;
and at the Museum.
Transcriber's Note
- Footnotes have been moved to the end of the article.
Featured Books

Wieland; Or, The Transformation: An American Tale
not disapprove of the manner in which appearances are solved, but that the solution will b...
Read More
Dorothy and the Wizard in Oz
ne of another strange adventure.There were many requests from my little correspondents for "more abo...
Read More
ABC of Fox Hunting
turned my Lord over.U. was the Upland, where we viewed the Fox in.V. was the very last field—just ...
Read More
Maiwa's Revenge; Or, The War of the Little Hand
about two thousand acres of shooting round the place he had bought inYorkshire, over a hundred of w...
Read More
Rupert of Hentzau: From The Memoirs of Fritz Von Tarlenheim
R OUR LOVE AND HER HONOR CHAPTER XX. THE DECISION OF HEAVEN CHAPTER XXI. T...
Read More
The Head of Kay's
I — MAINLY ABOUT FENN "When we get licked tomorrow by half-a-dozen wickets," sai...
Read More
The Devil's Dictionary
ime, too, some of the enterprising humorists of the country had helped themselves to such parts...
Read More
Stories by English Authors: The Orient (Selected by Scribners)
ll complete. But, to-day, I greatly fear that my King is dead, and if I want a crown I mus...
Read More
Comments on "A Bilateral Division of the Parietal Bone in a Chimpanzee; with a Special Reference to the Oblique Sutures in the Parietal" :